More than fifty experts met in Xi’an, China, for an international academic conference on demographic change and social development last week. Several scholars from the Freeman Spogli Institute for International Studies (FSI) spoke at the conference, including Karen Eggleston, Marcus Feldman, Jean Oi and Scott Rozelle.
The conference marked the 120th anniversary of Xi’an Jiaotong University’s founding and more than three decades of collaboration with Stanford scholars. Researchers at Xi’an Jiaotong University’s Institute for Population and Development Studies collaborate on policy-relevant research and educational activities with Stanford faculty at FSI as well as the Morrison Institute and Woods Institute.
For more information on FSI’s work in the areas of global health and medicine, please visit this page and the Asia Health Policy Program website.
In a Q&A, Stanford postdoctoral fellow Darika Saingam explains why Thailand's battle against drugs continues and what is needed to introduce good policy that works to prevent illegal drug trade and supports recovering addicts.
Despite Thailand’s decade-long crackdown on drugs, demand for illegal substances has risen. A green leaf drug known as ‘kratom’ is a symbol of this rise as young people eagerly adopt the drug for entertainment and join an older generation of laborers who chewed it to survive long hours of work in the fields—and are now heavily addicted. Curtailing substance abuse and its consequences takes good public policy and solutions must be area-specific and evidence-based, according to a Stanford postdoctoral fellow.
Darika Saingam, the 2015-16 Developing Asia Health Policy Postdoctoral Fellow, has conducted two cross-sectional surveys and more than 1,000 interviews with drug users, recovered addicts, and local public officials in an effort to better understand the evolution of substance abuse in southern Thailand.
At Stanford, she is preparing two papers that offer policy options suitable for Thailand and other developing countries in Southeast Asia. Saingam spoke with the Shorenstein Asia-Pacific Research Center (APARC) where she will give a public talk on May 17. The interview text below was edited for brevity.
For decades, Thailand has been an epicenter of drugs. Can you describe the extent of the problem today?
According to a 2014 report, 1.2 million people were involved in illegal drug activities across Thailand. The total number of drug cases saw a 41 percent increase from 2013 to 2014. New groups of drug traffickers are mobilizing while existing groups are still active. Drug users who are young become drug dealers as they get older. The number of drug users below 15 years of age has increased dramatically.
According to your research, what drives Thais toward illegal drug use and the trafficking business?
Adults in Thailand use drugs to relieve stress and counteract the effects of work. Adolescents use them for entertainment. Historically, farmers and laborers from rural areas of Thailand would use opium for pain relief. More recently, a consumable tablet known as yaba has become popular along with crystal methamphetamine and marijuana. Young people are increasingly using yaba and kratom.
Thailand is still a developing country, but it is industrializing quickly. Social and cultural norms have been shifting and people want an improved quality of life. A lot of young people are unemployed and lack social support and are therefore more likely to turn to drug trafficking for economic opportunity. The economic recession and political strife in countries bordering Thailand have exacerbated the situation.
Image
Image
Photos (left to right): A man holds up a kratom leaf. / Saingam examines kratom leaves as part of her research to understand illegal cultivation practices.
What is kratom and why is it popular?
For nearly a century, the native people of Thailand have chewed kratom. It is a leaf that grows on trees resembling a coffee plant. Historically, kratom was used to reduce strain following physical labor, to be able to work harder and longer, and to better tolerate heat and sunlight. Kratom is also embedded in Thai culture and given as a spiritual offering in religious ceremonies. My field research in the southern province of Nakhon Si Thammarat has shown that these motivations are still true today.
Within the past seven years, kratom use has skyrocketed and people are using it in increasingly harmful ways. Chewing kratom is not immediately harmful to health, but combining it with other substances is. This is the recent trend. Users have created new ways to consume it such as in a drink known as a ‘4x100.’ It contains boiled kratom leaves, cough syrup and soft drinks. Additional methamphetamines and benzodiazepines are sometimes added to that mixture.
What strategies must be employed to control substance abuse?
The first step is to realize that the patterns of substance abuse are specific to each location therefore solving the problem must also be. Drug usage is also dynamic. Placing hard control measures on one substance often provokes the emergence of another in its place therefore a holistic approach is important.
Thailand should employ multiple strategies toward effective prevention and control of substance abuse. These strategies include examining the problem and creating policies from an economic perspective (supply and demand), an institutional perspective (national and international drug control cooperation), and a social perspective (structural supports for recovered addicts and mobilization of public participation).
What is the Thai government doing to address the drug problem, and what could they be doing better?
Politicians in Thailand must do a better job at representing the people. Government health workers are often gathering information, assessing needs, and reporting findings to politicians, but these needs are not being accurately addressed. An example of this is politicians ordering to cut down kratom trees – a public display that does not get at the root cause of the problem. The reality is that drug users will quickly find substitutes. According to my study, of the regular users that stopped using kratom, more than 50 percent turned to alcohol instead and did so on a daily basis. This is merely a shift from one substance to another.
On the upside, a crop substitution program created under King Bhumibol Adulyadej offers a successful working model. The program works to replace opium poppy farming with cash crop production. It began in 1969 and is cited for helping an estimated 100,000 people convert their drug crop production to sustainable agricultural activities. Crops cultivated can be sold for profit in nearby towns. The program has also introduced a wide variety of crops and discouraged the slash-and-burn technique of clearing land. It is win-win because it stymies drug trade and provides economic opportunity while also being ecologically sound. This type of program should continue to be scaled up.
Can this model be co-opted elsewhere? What lessons from other countries could inform Thailand’s approach?
Yes, the model could plausibly be implemented in other areas in Thailand and in other Southeast Asian nations.
I think a judicial mechanism such as the kind seen in France could benefit the rural areas in Thailand. The French government has established centers across the country that act as branches of the court that try delinquency cases of minor to moderate severity, and also recommend support services for drug users. Members of the magistrate and civil society actors manage center operations thus placing some responsibility back onto the local community.
I believe an opportunity also exists for Thailand to legalize kratom. Legalization would show a respect for the cultural tradition of chewing kratom leaves and allow the government to suggest safer ways of using it. Bolivia has created a successful model of this through its legalization of coca leaves. Coca in its distilled form is cocaine, but left as a leaf, it is not a narcotic. Indigenous peoples are allowed to chew coca leaves. The government policy is being credited for a decrease in cocaine production as well.
Hero Image
Stanford postdoctoral fellow Darika Saingam conducts interviews and collects data in southern Thailand. | All photos courtesy of Darika Saingam
What is the best way to measure returns on investments in health care?
Does the World Health Organization’s approach help developing countries allocate their limited health-care resources wisely?
What are the economic implications of the global rise in non-communicable diseases?
These are just a few of the global challenges taken up by health economics experts at the third annual Global Health Economics Consortium Colloquium at the University of California, San Francisco.
At the core of the conference is the growing field of health economics, and why cost-effectiveness analysis is fast becoming the underpinning of successful health policies.
“It’s been great to see the meeting evolve from a show-and-tell to a platform where we can have nuanced discussions about the challenges and controversies in the field,” said Dhruv Kazi, an assistant professor of medicine at UCSF who helped organize and moderate the event.
Some 180 health policy experts, researchers and speakers representing 11 universities, six non-profit organizations and five for-profit outfits attended the daylong conference on the UCSF Mission Bay campus.
“By building bridges between our universities, we create a space where thought-leaders and students alike can engage in discussions to challenge working assumptions and also spearhead innovate strategies and solutions,” said James Kahn, a professor of health policy and epidemiology at UCSF and the director of the consortium.
The Consortium — known as GHECon — was awarded a five-year cooperative agreement of up to $8 million by the CDC to conduct economic modeling of disease prevention in five areas: HIV, hepatitis, sexually transmitted diseases, tuberculosis and school health.
Taking a break during the third annual Global Health Economics Consortium Colloquium at UCSF on Feb. 13, 2016. Photo by UCSF/Cindy Chew.
As global economies remain turbulent, Kazi said, governments and donors have become increasingly cost-sensitive and want to better understand the societal returns they are getting for their investments in health.
“That enhances the influence of our work, but also increases the scrutiny it receives, creating an opportunity for the community to have an honest discussion about the challenges and opportunities that lie ahead,” he said. “And that is precisely the platform GHECon sees itself becoming.”
Some of the tough challenges consortium members are undertaking:
The World Health Organization recommends using per capita GDP as a benchmark for how much money countries should be willing to spend on health-care interventions. GHECon researchers have shown that this approach is problematic and does not always help countries allocate their limited health-care resources optimally.
Economic evaluations have typically only considered health-care costs, overlooking the lost income of patients or caregivers during hospital stays. GHECon researchers are working on ways to value this lost productivity in an effort to estimate the true cost of a disease and, conversely, the benefit of its alleviation.
Cost-effectiveness evaluations traditionally are concerned with how efficiently health-care resources are utilized by asking questions like: How many lives can I save per million dollars invested? But society may care about other benefits that go beyond efficient use of resources, such as reducing disparities by helping the most vulnerable sections of society and alleviating poverty.
He said there are two big challenges today: defining cost-effectiveness thresholds that are meaningful, and determining how policymakers, donors and payers make decisions when there are multiple criteria and perspectives.
“The realities of decision-making inevitably involve a whole host of considerations,” said Sculpher, who is director of the Program on Economics Evaluation and Health Technology Assessment at the University of York. “Ultimately it’s about what is this measure of benefit that we want to maximize — and how do we invest in it.”
Stanford Health Policy’s Douglas K. Owens, director of the Center for Health Policy at the Freeman Spogli Institute for International Studies and the Center for Primary Care and Outcomes Research at the Department of Medicine, presented his influential economic modeling research about the need for routine HIV screening.
“We determined that HIV screening is cost-effective in virtually all health-care settings,” Owens told the audience, noting that the findings became policy at the Centers for Disease Control and Prevention and other national health policy organizations. It has become an example of how economic modeling can inform crucial policy decisions — and help save lives.
There were also robust panel discussions about the challenges of doing cost-effectiveness analysis in developing countries with limited resources; the difficult paths to universal health care; and how economics can help address disparities in health care and financial protection.
“The consortium is particularly valuable because it fosters collaborations among a broad group of global health experts,” Owens said.
Image
Hero Image
Stanford Health Policy's Douglas K. Owens presents his influential economic modeling research about the need for routine HIV screening at the third annual Global Health Economics Consortium Colloquium at UCSF, Feb. 12, 2016. | UCSF/Cindy Chew
Jonathan H. Chen was an intern at Stanford Hospital a few years back, admitting patients with unusual medical syndromes or rare diseases.
He wasn’t always sure how to immediately treat these patients.
“I found myself clueless at times,” said Chen. “I thought to myself, I should review the chart of a similar patient who had an experienced clinician care for him so that I can learn from their care plan.”
That triggered Chen’s eureka moment.
“Why look at just one person’s chart?” he thought. “Why not look at the last thousand charts to see how all doctors take care of their patients in similar cases?”
Doing so, he would have the potential to crowd-source the collective wisdom of physicians all in one central location.
Already having a PhD in computer science and spending a few years as a software developer before medical school, Chen — a wunderkind who started college when he was 13 — knew he had the rare set of skills to marry medicine and technology.
“I thought about how the Amazon product-recommender algorithm works and thought, `Can we do this for medical decision-making?’” said the 34-year-old Chen, a VA Medical Informatics Fellow at Stanford Health Policy.
So instead of, other people who bought this book also liked this book, how about: Other doctors who ordered this CT scan also ordered this medication.
“What if there was that kind of algorithm available to me at the point of care?” he asked. “It doesn’t tell me the right or wrong answer, but I bet this would be really informative and help me make better decisions for my patients.”
The National Institutes of Health agrees. Chen was recently awarded a five-year NIH grant as the principal investigator behind OrderRex, a digital platform that data-mines electronic medical records to learn clinical practice patterns and outcomes to inform concrete medical decisions.
Chen is designing and coding OrderRex with the help of his chief mentor, Russ Altman, a professor of bioengineering, genetics and medicine and director of Stanford’s Biomedical Informatics Training Program. Stanford Health Policy professors of medicine, Mary Goldstein and Steven Asch, round out his core team of grant mentors. Grant collaborators Nigam Shah, Lester Mackey, and Mike Baiocchi are providing additional critical expertise.
“I think OrderRex is a first step towards an entirely new way to provide decision support to physicians,” said Altman. “We will not only have a large database of patients from which we can collect similar patients to create virtual cohorts, but we will also have a database of the decisions that their physicians have made in different clinical situations.”
Altman added: “Each of these capabilities would be transformative — but together they would really change what is possible for a provider sitting with a patient, making decisions about diagnosis and therapy.”
The NIH’s Big Data-to-Knowledge grant will allow Chen to develop and test the platform. Stanford Medicine’s Center for Clinical Informatics provided Chen a year’s worth of Stanford Hospital records, including every medical order for every patient. The more medical data he loads, the more patterns begin to form.
Chen has been using a derivative of Amazon’s algorithm to make his platform scalable with millions of patient records. The broad vision is to eventually integrate this tool with hospital computer networks to assist physicians with their decisions.
“Imagine, technology allowing medical decisions to be informed by the collective experience of thousands of other physicians right at the point-of-care,” Chen said.
There are naysayers who worry such a product will further alienate physicians from their patients and allow doctors to jump to crowd-sourced conclusions about treatment. Chen emphasizes OrderRex would only serve as a tool, which does not substitute for human contact, calculations and conclusions.
“Tools like this are simply to augment the medical decision-making process and hopefully — and I know this is a big goal — improve the quality and efficiencies of health care.”
Altman says the lacking-human-touch argument is imprecise and potentially unethical.
“Of course, providers will always be real people and of course they should be empathetic, listen to the patient, examine the patient, and think about what’s best in the big picture,” he said. “But if there are technological tools that they can use to improve their decision-making, it is probably unethical to replace data-driven decision-making with `touch’ and ‘intuition’ — which often perpetuates the status quo and contributes to variability in practice and variability in outcomes.”
Stanford Medicine is already leading the revolution in precision health and big data to overcome human error and misdiagnosis.
The idea is to give doctors access —a green button — to patient data from a vast collection of electronic medical records. They wrote that the instant access to EMRs isn’t a substitute for a clinical trials, but better than resorting to the physician’s own bias-prone memory of one or two previous encounters with similar patients.
Chen is working with those professors, but notes the Green Button concept is to look for “patients like mine” and ask questions about different treatment options that may yield different results. His approach looks for “doctors like me,” and anticipates what the doctor wants before they ask for it.
“The conceit of my approach is that all practicing doctors are already trying to make our best-guess decision to improve our patients' outcomes,” he said. “Rather than trying to directly predict how to change a patient outcome, I look to the records of physician decision-making that already represent a wealth of expertise we are not leveraging in a systematic way.”
Could that wealth of expertise one day make Chen a wealthy man, perhaps the Jeff Bezos of the medical informatics world?
“I wouldn’t complain if I was,” Chen said with a grin. “But if I just wanted to make money, I wouldn’t have gone to medical school,” He gave up a lucrative living as a software developer.
He does recognize, however, that for OrderRex to have a big impact, commercial applications such as licensing the product as an add-on to EMR systems are likely.
“So, having a broad impact that will serve the mission of improving quality and efficiency — that is the ultimate goal.”
Hero Image
Jonathan H. Chen, a VA Medical Informatics Fellow at Stanford Health Policy, works on his digital records platform, OrderRex, during a break in rounds at the VA Hospital in Palo Alto. | Joseph Matthews/VA Palo Alto
Every Halloween there seems to be another animated brushing campaign to save children from their own sweet tooths. For most, the goal is simple: better oral hygiene for kids.
PLAQUEMONSTER is different.
Developed by Jason Wang, director of the Center for Policy, Outcomes and Prevention (CPOP) and a Center for Health Policy/Center for Primary Care and Outcomes Research (CHP/PCOR) core faculty member, and his team, PLAQUEMONSTER does encourage children to practice good oral hygiene. However, the true purpose of the app is to provide feedback on the user’s engagement that can be used for future forays into mobile health.
Image
Smart phone users can download the application to create a “tooth pet” and help it grow by brushing and flossing daily. Neglect oral hygiene, and the tooth pet will grow dirty, become infected by “plaquemonsters,” and eventually end up in jail.
Using the game’s team mechanic, the app urges children to encourage their friends to brush and floss. Teammates can release a tooth pet from jail, so kids must hold each other accountable if they want their team to progress.
“The social aspect really does make a difference,” said Zara Abraham, a digital media specialist at CPOP and one of the app’s designers. She found that the app’s first child testers “would always be on the phone making sure that each one was doing their work, checking on their teeth.”
The social aspect is likely to engage children more than the average brushing and flossing campaign, according to Abraham. The app’s storyline also helps set PLAQUEMONSTER apart.
Image
“The storyline we came up with was really sticking it to the man,” said Abraham. Developers set tooth pet up as a heroic rogue character who does what he thinks is right by eating healthy despite pressure to give in to Big Candy. Facing peer pressure to subsist on a diet of candy but also more serious pressure from “candy corporation,” tooth pet must expose the company’s nefarious practices so that teeth can be clean again. The game’s darker aspects and complex storyline may help make the game more accessible to older children and hopefully will keep kids engaged longer.
However, PLAQUEMONSTER is more than just a game, more even than a campaign for oral hygiene. Wang’s team hopes to use health literacy games along with demographic and engagement information to develop other mobile health apps. Ultimately, PLAQUEMONSTER is a tool for discovering how people engage with health on a mobile platform and how mobile health apps can improve health care.
“The spirit that Jason brings to the app is the game mechanics of behavioral economics,” said Manuel Rivera, product manager at CPOP.
Eventually, Wang’s team hopes to develop other mHealth apps that could aid patients with serious conditions, helping them to track their health and engage in their care plan. Wang’s long-term goal is for “people who are of working age and elderly to improve their quality of life and health trajectories” using mobile health.
If all goes well, PLAQUEMONSTER could be a first step toward active engagement between patients and health care using mobile platforms.
This project is supported by an NIH Director's New Innovator Award.
Medical researchers must work together across disciplines to provide better health care to those who need it most, according to panelists at Stanford Medicine’s Annual Population Health Sciences Colloquium.
The symposium, hosted by the Stanford Center for Population Health Sciences, brought together working groups from across the Stanford campus to showcase the latest findings in population health research.
“Population health science at Stanford is likely to make the most important contributions when we cross traditional intellectual expertise disciplines,” said Paul H. Wise, a core faculty member at the Center for Health Policy/Center for Primary Care and Outcomes Research (CHP/PCOR).
Many of the scholars at the daylong conference on Tuesday stressed that an interdisciplinary approach to health care is crucial to understanding and aiding underserved populations.
“To deal with life-course questions we need to create-life course observational windows,” said Mark Cullen, chief of the Division of General Medical Disciplines and director of the Stanford Center for Population Health Sciences.
Instead of trying to create an all-encompassing care plan for the human population as a whole, panelists demonstrated that studying the needs of particular groups, or smaller populations, can better serve individuals within populations that may not receive the best care.
Douglas K. Owens, director of CHP/PCOR, said the U.S. Preventive Services Task Force, of which he is a member, has “often faced a real paucity of data trying to develop prediction guidelines for both the very young and the old.”
The Task Force, a panel of experts that makes recommendations for medical prevention services, is generally able to make guidelines for large populations like adults, but suggestions for specialized groups like children and the elderly are more challenging. Though Stanford researchers like Wise are working to improve care for particular sectors like children, more study is needed.
Several speakers at the conference said the underserved population of poor children could benefit from research targeted toward their population group.
“We don’t really understand the biology of the life-course, why things taking place in gestation and early life actually affect healthy aging and adult onset disease,” said Wise, adding, “We have a very poor understanding of how to translate this understanding into effective interventions for communities in need.”
Panelists agreed that big data can help them understand smaller, poorly served populations, such as young children in impoverished communities. By collecting large amounts of data from the general population, researchers will increase the amount of data available for more specific groups. This allows researchers to study these populations more closely and help create better outcomes.
Abby King, a professor of health research and policy and of medicine, and Jason Wang, director of the Center for Policy, Outcomes and Prevention (CPOP) and a CHP/PCOR core faculty member, believe life-course digital applications can provide individualized care while collecting data on a large-scale.
According to King, a life-course app, or a device to track health and provide care throughout one’s life, would grow with the user and help them through important developmental stages.
Image
Wang has taken a first step toward creating such an app with PLAQUEMONSTER. Intended for children eager for Halloween candy, the PLAQUEMONSTER app provides kids with a “tooth pet” they must keep safe from “plaquemonsters” and the so-called evil candy corporation. By flossing and brushing their teeth each day, kids earn points, and Wang’s team hopes the game will encourage good dental hygiene.
Health-care techniques using mobile devices, known as mHealth, could be particularly useful in underserved populations. King notes that even low-income populations have cell phones, so using phones as health-care tools could help decrease the gap between higher- and lower-income populations.
“I think for us one of the major challenges of the century is to really close that health-disparities gap and mHealth can help.”
However, each app must be tailored to the user.
“There’s no reason to believe that an African-American 16-year-old is going to be motivated the same way as a 45-year-old white man,” said Wang. “You need to involve patients in the design of the app.” When the app fits the specific patient’s needs, they are more likely to use it regularly, and knowing the needs of their population helps determine their preferences.
As the world continues to become more connected, the panelists said that reaching across disciplines and incorporating technology may hold the key to effective health care in the 21st century.
Foreign aid to the public health sectors of developing countries often appears to be allocated backwards: The global burden of non-communicable diseases such as diabetes or heart disease is enormous – yet they receive little health aid.
By comparison, the global burden of HIV is much smaller, yet it receives more health aid than any other single disease.
So will a wholesale reversal in health aid priorities improve global health? The answer, according to a new study by Stanford researchers, is that if the goal is to maximize the health benefits from each donor dollar, health aid is actually allocated pretty well.
Still, reallocating foreign aid to step up the fight against malaria and TB could lead to greater overall health improvements in developing nations. And it could be done without spending more money, the researchers have found.
Eran Bendavid, an assistant professor in the Department of Medicine and a core faculty member at the Center for Health Policy and Center for Primary Care and Outcomes Research, and three Stanford research assistants write in the July issue of Health Affairs that more health aid is going to disease categories with more cost-effective interventions.
"What we found, somewhat to our surprise, is that in nearly all countries, more aid was flowing to finance priorities with more cost-effective options,” Bendavid said in an interview. “That is partly because more aid was flowing to the treatment and prevention of infectious diseases such as HIV and malaria, and their management can be relatively inexpensive, even if the burden of these diseases is lower than that of non-communicable diseases.”
Bendavid, an infectious disease physician, added: “Conversely, even though the burden of non-communicable diseases is high and growing, addressing these chronic conditions such as diabetes and heart disease is, broadly, more costly than the unfinished infectious disease agenda.”
The authors also show that just because health aid is broadly allocated toward better cost-effectiveness does not mean that it cannot be better allocated.
The biggest gains would come from taking some of the foreign aid earmarked for HIV or maternal, newborn or child health, and putting it toward programs to treat malaria and tuberculosis, they write.
The Stanford research team reviewed the literature for cost-effectiveness of interventions targeting five disease categories: HIV, malaria, tuberculosis, non-communicable disease and maternal, newborn and child health.
What they found was that aid from wealthy nations to developing ones might be allocated efficiently, but that the money is not always spent in the best interest of curbing the communicable diseases that would improve the overall health of a nation.
It is crucial, therefore, to further study the consequences of realignment of donor funds.
Public health aid is critical to most developing countries. Development assistance from high-income countries to public health sectors of low- and middle-income countries amounts to nearly 40 percent of public health spending in countries with a per capita GDP of less than $2,000.
The researchers focused on 20 countries that received the greatest total amount of aid between 2008 and 2011, a period of historically unprecedented growth in health aid. Development assistance has since flattened, however, so the authors believe it’s increasingly important to consider best value when investing limited resources.
The 20 countries studied – from Afghanistan to Zambia – received $58 billion out of the total $103.2 billion in recorded health aid disbursements to 170 countries between 2001 and 2011.
“Over the period of 2001-2011, a greater amount of disbursements flowed to HIV programs than any other disease category,” the authors write. “On average, interventions addressing malaria and had the lowest incremental cost-effectiveness ratio (ICER), which indicates that malaria interventions could yield greater health improvements from each dollar compared with the interventions having a higher ICER.”
The authors analyzed the data and determined that the alignment improves if up to 61 percent of HIV aid is reallocated for TB control and up to 80 percent is reallocated for malaria control.
“Our evidence suggests that the greatest improvements in the efficiency of global health dollars could result from reallocating funds to malaria and TB control programs,” the authors write.
“This study shows, for the first time, that the current allocation of health aid is generally aligned with the cost-effectiveness of targeted interventions. Contrary to common views that advocate for reprioritization toward non-communicable diseases, our data suggest that the alignment could best be improved by focusing on malaria and TB, especially where addressing those diseases is highly cost effective.”
The other authors of the study are Andrew Duong and Gillian Raikes, both research assistants in the Program of Human Biology; and Charlotte Sagan, a RA in the School of Medicine.
The increasing resistance to antimicrobial drugs is a growing public health concern, particularly in low- and middle-income countries that require high out-of-pocket payments for prescription drugs.
“Understanding the drivers of antibiotic resistance in low- to middle-income countries is important for wealthier nations because antibiotic-resistant pathogens, similar to other communicable diseases, do not respect national boundaries,” said Marcella Alsan, MD, PhD, MPH, the lead author of the study, which was published July 9 in The Lancet Infectious Disease.
“Out-of-pocket health expenditures are a major source of health-care financing in the developing world,” said Jay Bhattacharya, MD, PhD, senior author of the study and a professor of medicine, a senior fellow at the Freeman Spogli Institute for International Studies and another core faculty member at CHP/PCOR.
Yom Nob, a lab technician at Ta Sanh Health Center, Cambodia sends a text message to a new drug resistance alert system. The WHO and its partners use the alert system to map and track drug resistant cases of malaria. | The Gates Foundation
China was for hundreds of years almost entirely an agricultural society, but modern industrialization changed that dynamic, and the impact on health has been startling.
Urbanization, population aging and changes in lifestyle (from mobile to sedentary) have led a transition from an acute to chronic disease-ridden society. Now, 10 percent of China’s adult population is diabetic or pre-diabetic—holding the number one place in the world.
Feng Lin and a team of researchers want to change that reality.
Lin is part of the Corporate Affiliates Program at the Shorenstein Asia-Pacific Research Center. A visiting fellow, Lin leads a research project focused on innovations in primary health care systems in China, a topic that is also the core of his work at ACON Biotechnology. Throughout his research, Lin has worked with health policy expert Karen Eggleston.
“Thirty to forty years ago, people were talking about infectious disease,” Lin says, referring to Chinese society. “Non-communicable diseases (NCDs) like diabetes didn’t even register. They were like the black sheep in the flock.”
Now, though, Lin says that China has reached a critical stage. NCDs have a noticeable presence, and the challenge for China is to create an effective healthcare system to serve its population of 1.3 billion. Its health delivery systems are not equipped to address and prevent diseases at such a high demand.
Lin believes that improving access to care by increasing the relevance of community health care centers, improving the quality of care and integrating IT infrastructure could provide pathways forward.
In pursuit of this, he is part of the team developing an open source health index with Yaping Du, a professor at Zhejiang University, and Randall Stafford, a professor of medicine at the Stanford Prevention Research Center.
The index is one of many activities that Lin is involved with at Stanford. Forging a new type of partnership with the Asia Health Policy Program, his company sponsored a public seminar series this past year.
Determining how to restructure China’s healthcare system is a tough challenge because it’s a bureaucratic hierarchy – multiple divisions traverse each province, prefecture, township and village.
In 2009, the Chinese government laid out aggressive reforms to its healthcare policy. Lin says he believes the most essential part of that plan is the empowerment of grassroots-level community healthcare centers.
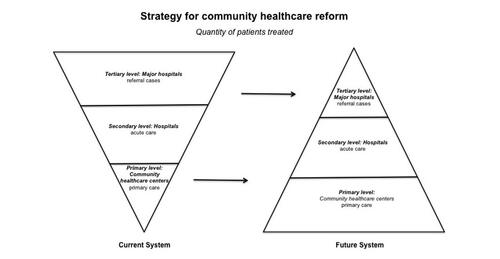
“You cannot just deal with primary level, you must look at the secondary and tertiary segments, too—a whole system approach,” he says.
Resembling a pyramid, China’s system has a finite number of top physicians who are mostly located at major hospitals. Patients who pursue services are likely to go to major hospitals in urban areas, instead of their local health community centers. About 90 percent of health care is delivered in hospitals—leading to overcrowding. Moreover, patients choose to self-treat or self-medicate which can lead to misdiagnosis.
Collecting data in Hangzhou, a coastal city just south of Shanghai (shown in map photo), Lin discovered that these trends could be explained by two reasons.
Patients have a low level of trust in community health centers, and local facilities lack capacity (e.g. having only 20 bed spaces) and expertise (e.g. employing medical personnel with sometimes outdated training). His analysis reinforced earlier outcomes found by Karen Eggleston.
Lin says the solution lies in increasing access to highly skilled physicians and organizing the system more efficiently.
Comparing China to the United States, Lin believes community healthcare centers should become main hubs for service delivery. The centers would operate as the first and last touchpoint for patient care, like “gatekeepers” in the U.S. system, administering advanced services and prevention programs like wellness education.
And while local centers are becoming more prevalent—China has more than 34,081 centers—development isn’t fast enough, not enough physicians exist, and patients aren’t actively choosing to redirect their services to community healthcare centers.
Courtesy: Feng Lin
Figure 1. Strategy for community healthcare center reform advocates "strength at the grassroots." Currently patients seek care at major hospitals as their first stop, but in the future system, patients will go primarily to grassroots community healthcare centers. Courtesy: Feng Lin
Creating ease
Chinese people are typically leery of the quality of health care available at community healthcare centers, and overcoming that trust deficit won’t be an easy task. However, Lin says it’s a matter of informing citizens about local services and training more physicians to deliver quality care.
To address quality concerns, the Chinese government has set out to expand medical training programs. Enhancing the expertise of current and future physicians in rural community healthcare centers is essential, Lin says.
The health index aims to empower patients so that they can determine the best medical accommodation available, and also create a mechanism that rewards good work.
The key is to create a participatory system, one that incentivizes the patient and the physician, he says.
Hosted digitally and in the public domain, the index will list all physicians throughout Zhejiang province. Patients and healthcare professionals can login and share their experience, providing a “satisfaction rating” of hospitals and community health care centers.
Beyond external contributions, the index will support data provided by China’s national Center for Disease Control and Prevention, and local centers for disease control, to include mortality rate and cause of death and many other indicators sourced from publicly available data.
“It will build up a kind of system that people can trust – something that people can rely on,” Lin says.
Similar platforms have been implemented in advanced industrialized nations. Lin hopes that the index will offer a model that could be applied nationwide.
“It’s nearly impossible to have a single policy apply,” he says. “But, if there’s a success in one area or a few areas, the central government will pick up that approach.”
Lin expects that his team will unveil the pilot program at a conference on general practice in October 2015. The conference aims to provide practical ways to improve primary care services and the education and training of general practitioners.
Noncommunicable diseases (NCDs) have become the leading causes of death worldwide and China's increased NCD prevalence is of growing concern. Randall Stafford, Professor of Medicine in the Stanford Center for Research in Disease Prevention and SCPKU Faculty Fellow, led a symposium at the center last fall. Entitled "Tackling China's Noncommunicable Diseases: Shared Origins, Costly Consequences, and the Need for Action," the symposium focused on China's NCD threats to public health and the urgent need for solutions. The symposium summary was published earlier this month in the Chinese Medical Journal.




 Taking a break during the third annual Global Health Economics Consortium Colloquium at UCSF on Feb. 13, 2016. Photo by UCSF/Cindy Chew.
Taking a break during the third annual Global Health Economics Consortium Colloquium at UCSF on Feb. 13, 2016. Photo by UCSF/Cindy Chew.












 Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
 Courtesy: Feng Lin
Courtesy: Feng Lin

